Shoulder injury related to vaccine administration (SIRVA)
What is it?
Shoulder Injury Related to Vaccine Administration (SIRVA) is a rare but serious complication following suspected inadvertent administration of a vaccine too high in the deltoid or into the shoulder joint. This may cause a local inflammatory response and potential trauma to local structures within the shoulder joint including bursae, ligaments and tendons resulting in sudden onset shoulder pain and restricted movement. Symptoms can last for weeks to months or as long as years. Affected individuals can experience varying degrees of disability which can impact on their activities of daily living, social and emotional wellbeing.
Symptoms
Distinguishing symptoms/features of SIRVA include:
- sudden onset shoulder pain within 48 hours of vaccination- different to the injection site pain expected following vaccination
- restricted range of movement (RROM) of affected shoulder
- persistent shoulder pain and RROM lasting >1 week, lasting weeks to months
- suspicion of incorrect vaccination site – too high in the upper arm.
Impacts and implications
The impacts of SIRVA can include:
- interrupted sleep due to pain
- difficulty with personal care, care of others and activities of daily living
- inability to participate in sports or hobbies
- modified work duties
- time off work related to symptoms and/or treatments and investigations
- loss of income due to time off work
- financial burden due to cost of treatments and investigations
- emotional and social wellbeing.
Further implications for an individual with SIRVA can include vaccine hesitancy, reduced confidence in healthcare/immunisation providers and the potential for impaired immunogenicity.
Diagnosis
A GP, specialist or allied health professional such as a physiotherapist can diagnose SIRVA based on presenting symptoms and clinical history following an immunisation.
If radiological investigations such as ultrasound or MRI are undertaken to support or confirm a diagnosis, abnormalities including bursitis, adhesive capsulitis, impingement syndrome, synovitis or tendon tears may be identified.
Early diagnosis of SIRVA leads to timely treatment which is thought to lessen the duration and severity of symptoms.
Treatment options
SIRVA can be treated in a variety of ways and may include any of the following:
- over the counter pain/anti-inflammatory medications
- prescription pain/anti-inflammatory medication
- oral corticosteroids
- corticosteroid joint injections
- physiotherapy or other allied health professionals
- massage
- surgery(rare).
How to prevent SIRVA
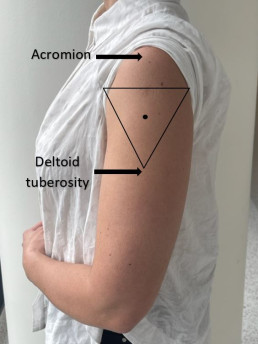
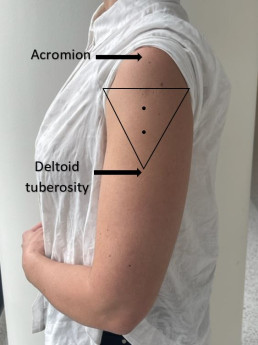
SIRVA can be prevented by following the recommended vaccination procedures for correct injection technique.
| Expose | Identify | Imagine | Inject |
| Expose the whole upper arm | Identify upper and lower anatomical landmarks (acromion and deltoid tuberosity) | Imagine an inverted triangle 2-3 fingers below the acromion | Inject vaccine in the centre of the triangle into the deltoid muscle |
Please refer to MVEC: Administration of injected vaccines- correct technique for further information on correct injection technique.
Where to report a case of SIRVA
All confirmed or suspected cases of SIRVA should be reported to SAEFVIC (the Victorian vaccine safety service). Reports can be made by consumers, immunisation providers or treating healthcare professionals.
SAEFVIC can provide clinical advice or facilitate consultation with an immunisation specialist if required.
Resources
- MVEC: Administration of injected vaccines- correct technique
- MVEC Education portal eLearning package: Shoulder Injury Related to Vaccine Administration (SIRVA)
- Australian immunisation handbook: Avoiding shoulder injury related to vaccine administration
- SIRVA (Shoulder injury related to vaccine administration); A case series- “Are you on target?”
- Cross GB, Moghaddas J, Buttery J, Ayoub S, Korman TM. Don’t aim too high: Avoiding shoulder injury related to vaccine administration. Aust Fam Physician 2016;45(5):303-306
- D. R (2023) Shoulder injury following COVID-19 vaccine administration: a case series and proposed diagnostic algorithm, Expert Review of Vaccines, 22:1, 299-306
Authors: Mel Addison (SAEFVIC Research Nurse, Murdoch Children’s Research Institute), Rachael McGuire (SAEFVIC Research Nurse, Murdoch Children’s Research Institute), Georgie Lewis (SAEFVIC Clinical Manager, Murdoch Children’s Research Institute) and Nigel Crawford (Director SAEFVIC, Murdoch Children’s Research Institute)
Reviewed by: Mel Addison (SAEFVIC Research Nurse, Murdoch Children’s Research Institute)
Date: March 23, 2023
Materials in this section are updated as new information and vaccines become available. The Melbourne Vaccine Education Centre (MVEC) staff regularly reviews materials for accuracy.
You should not consider the information in this site to be specific, professional medical advice for your personal health or for your family’s personal health. For medical concerns, including decisions about vaccinations, medications and other treatments, you should always consult a healthcare professional.